An ostomy is a surgically created opening made into the bowel or urinary tract for the purpose of eliminating waste materials (stool/urine) from the body.
The digestive tract is a hollow tube which stretches from the mouth to the anus and is lined with mucous membrane. As food and liquids travel through the system, enzymes are added which break down the food into a form that can be absorbed and used by our bodies. It is important to remember that digestion and absorption of nutrients takes place in the small bowel. The main function of the colon is to extract fluid and salt from the stool and act as a storage organ.
An ostomy is created to overcome problems with the bowel or bladder which are caused by injury, disease or congenital defect. All ostomies allow for the discharge of normal waste through a surgically created opening (stoma) in the abdomen. Most people with an ostomy wear a discreet odor proof pouch to cover the stoma and to collect body waste. An ostomy can be permanent or temporary.
In Canada about 13,000 ostomy surgeries are performed each year. It is also estimated the there are over 165,000 Canadians with an ostomy.
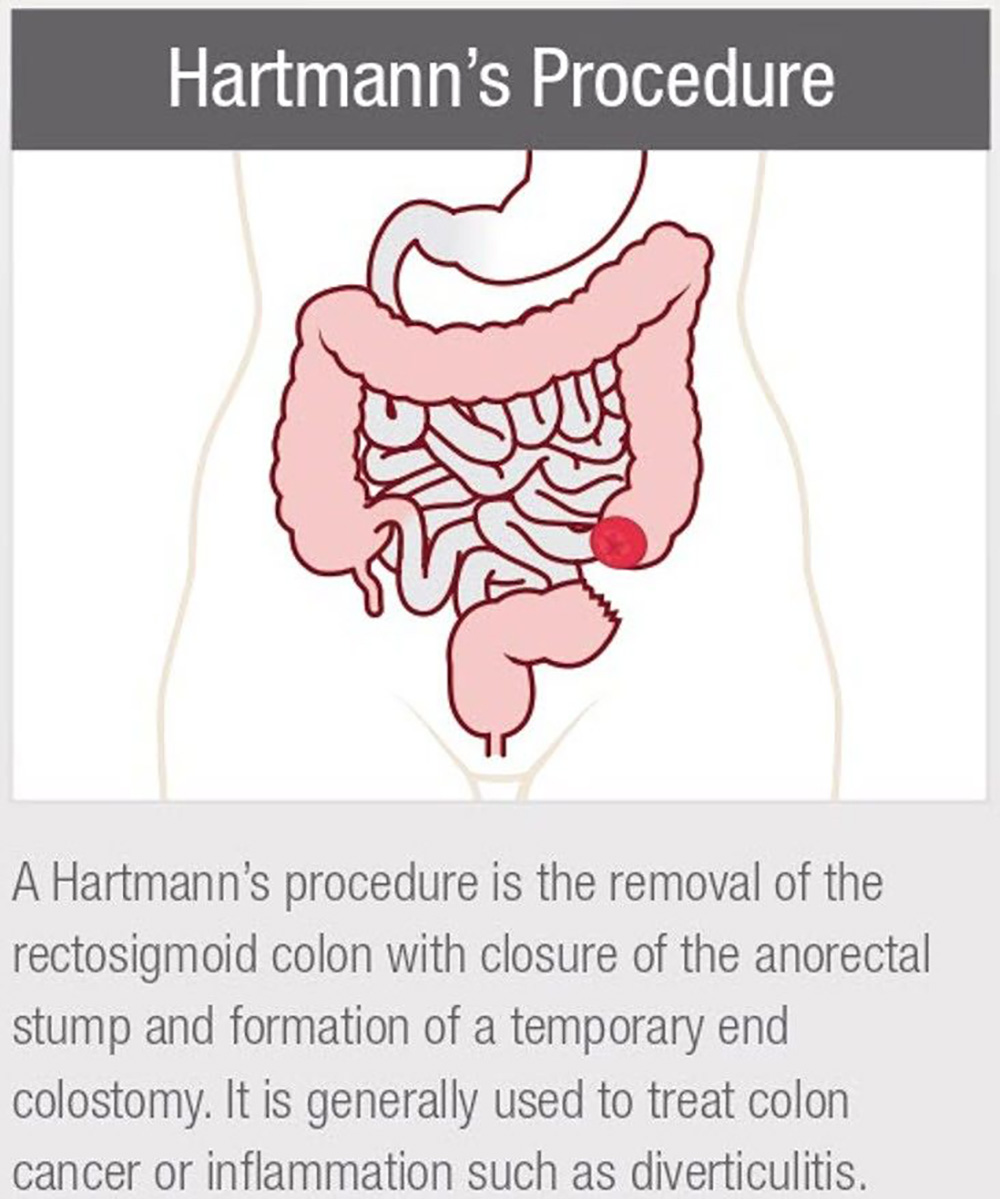
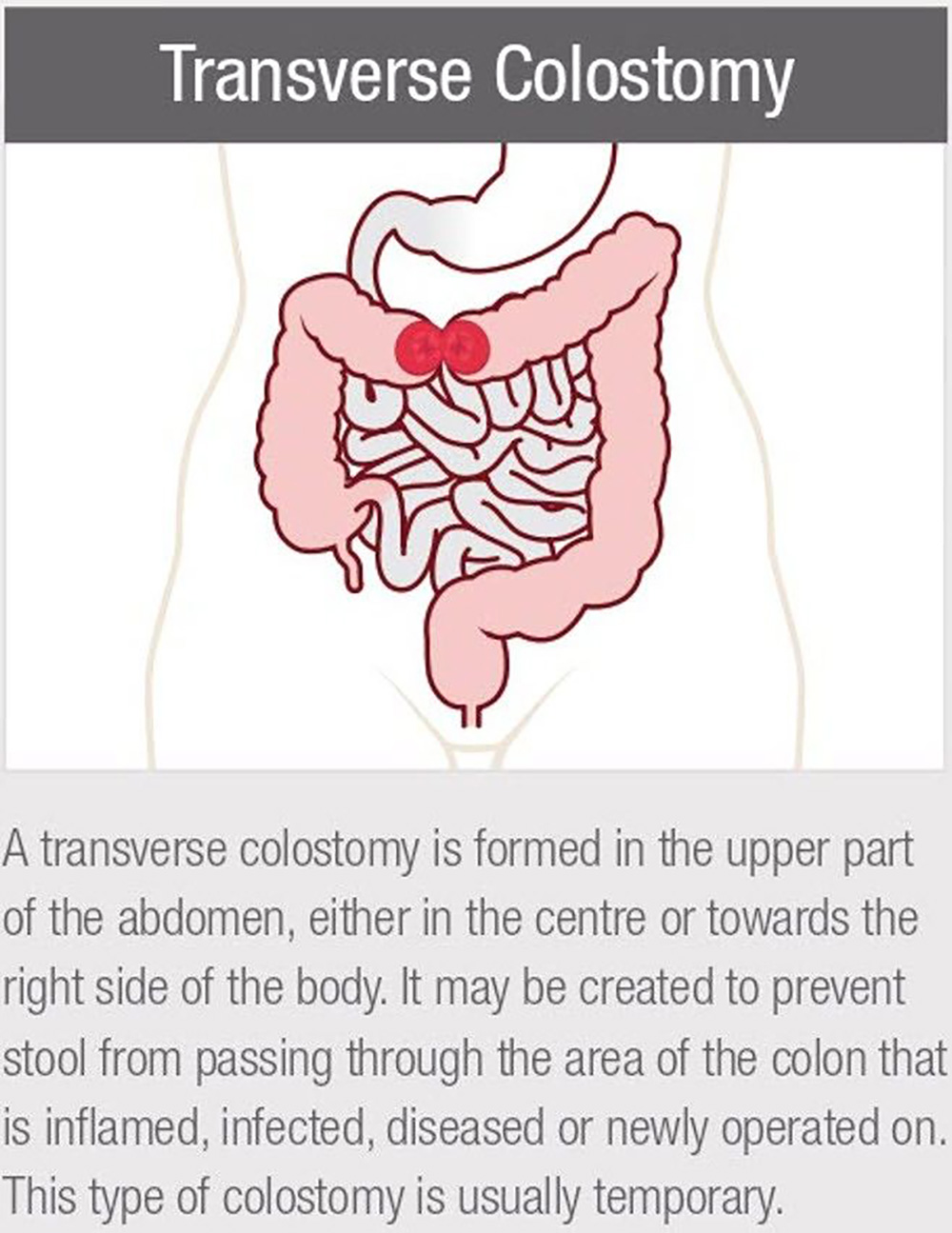
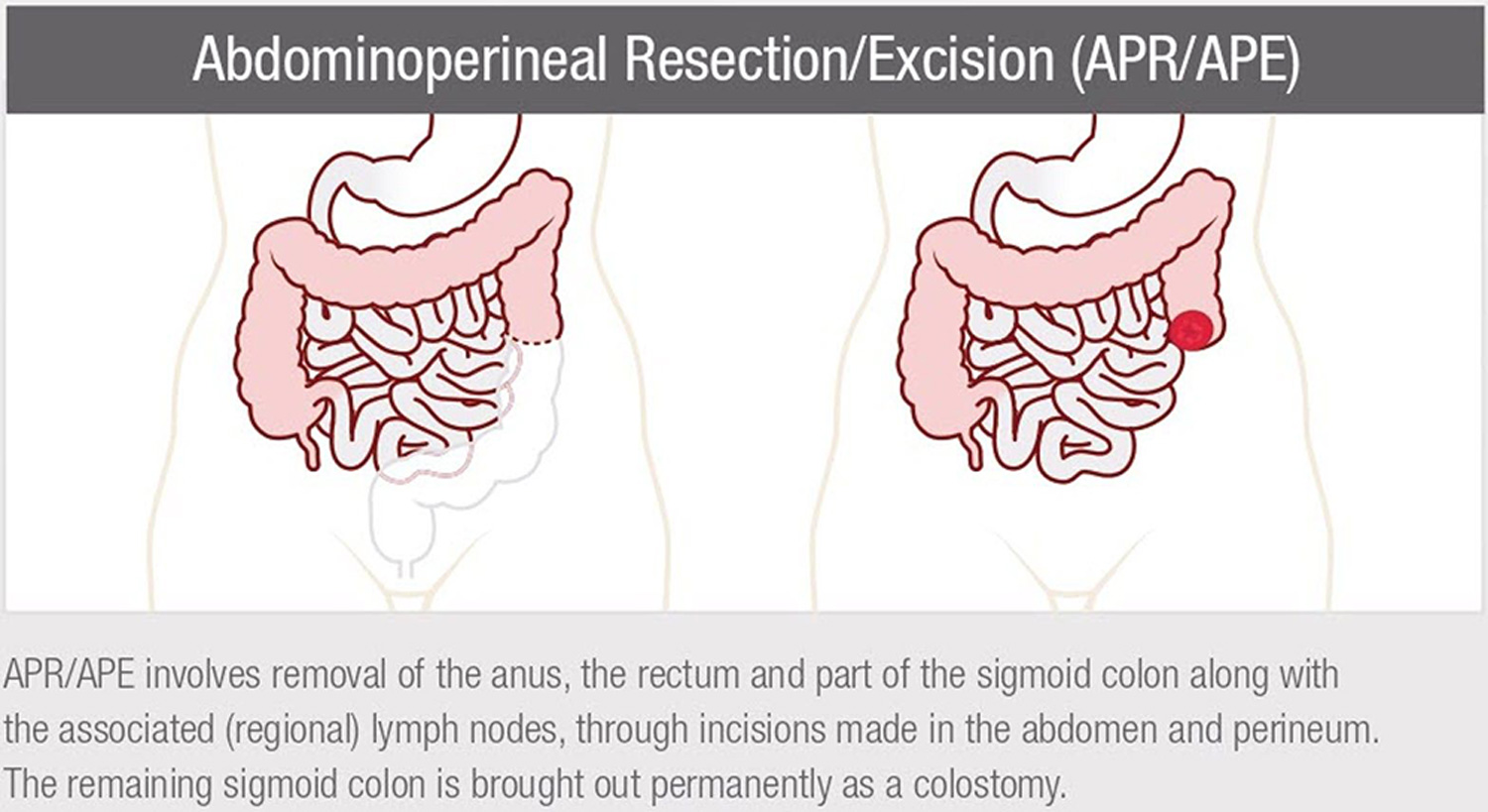
A colostomy is a surgically created opening in the abdomen through which a small portion of the colon (large bowel or intestine) is brought up to the surface of the skin creating a stoma. This allows stool to pass directly out of the body. A colostomy may be permanent or temporary.
Indications:
cancer
trauma
obstruction
Inflammatory Bowel Disease (IBD)
congenital malformations
abscess, fistulas, perforations
Output:
Varies depending on location of the stoma. The closer the stoma is located to the anus such as in the sigmoid colon, the more formed the stool. A stoma in the ascending colon will have a mushy consistency of stool.
Consistency of output will vary from mushy to formed stool. Flatus (gas) will also be passed through the stoma.
A guide to living with a colostomy
Credit: Nurses Specialized in Wound, Ostomy and Continence Canada
Surgically created opening in the abdomen through which the end of the ileum (small bowel or intestine) is brought up to the surface of the skin creating a stoma which allows waste to pass directly out of the body.
Indications:
· congenital malformation
· cancer
· trauma
· familial polyposis
· Inflammatory Bowel Disease (Ulcerative Colitis, Crohn’s disease)
Discharge:
· Liquid or paste consistency with gas.
· Drainage may change colour in response to certain foods.
· The waste (stool) contains residual digestive enzymes so it may be irritating to the skin.
A guide to living with an Ileostomy
Credit: Nurses Specialized in Wound, Ostomy and Continence Canada
Urinary diversion is a general term applied when the bladder is removed or the normal urinary structures are being bypassed. A surgical opening that creates a stoma is made in the urinary system to move urine flow away from the bladder. There are several surgical procedures to divert urine including the ileal conduit, ureterostomy (stoma created using a ureter), and continent urostomy (internal pouch).
Indications:
cancer
ongenital malformation (i.e. birth defects such as spina bifida)
spinal cord injury
damage or injury to urinary tract
neurogenic bladder
Output:
Urine, which may be pink with blood initially
Continuous drainage following surgery
Some mucus shreds in the urine
Ileal Conduit
This is the most common type of surgical urinary diversion. A 6” segment of the ileum (small bowel) is separated from the small bowel with the blood supply intact. One end of the segment is sutured closed, and the other end of the segment is brought out of the abdomen and a stoma is created. The ureters are implanted into this ileal segment. This serves as a passageway (conduit) for the urine. The bladder is removed or bypassed.
More information is available on Bladder Cancer Canada
Depending on the specific type of surgery, it may be called pelvic pouch procedure, J-pouch, S-pouch, ileoanal anastomosis, ileal pouch anal anastomosis (IPAA). With this type of surgery, the diseased colon (large bowel) and the inside layer of the anus (mucosa) are removed. Then, an internal pouch is constructed from a segment of the small bowel (ileum). This pouch and lower segment are surgically connected to the remaining rectal segment of bowel. This procedure allows for the use of the anal sphincter muscles to be maintained so the patient can have control to release stool as before. A temporary ileostomy is often created giving the reservoir (internal pouch) healing time.
Indications:
ulcerative colitis
familial polyposis
Output:
liquid to semi-formed stool
Continent Ileostomy
Is created when an internal pouch is constructed using the small bowel. A valve is surgically created where the pouch attaches to the abdominal wall. The valve prevents waste from being excreted out until the person drains the pouch using a catheter. Referred to as a “Kock Pouch” after the surgeon who created it. This surgery became less popular with surgical advances to create an ileal pouch anal anastomosis (IPAA) where the waste is passed out of the body through the anus.
Indications:
ulcerative colitis
familial polyposis
Output
Using a special catheter inserted into the stoma, the pouch is drained of waste four or five times a day. Stool will be a liquid or mushy consistency.
What is a Stoma?
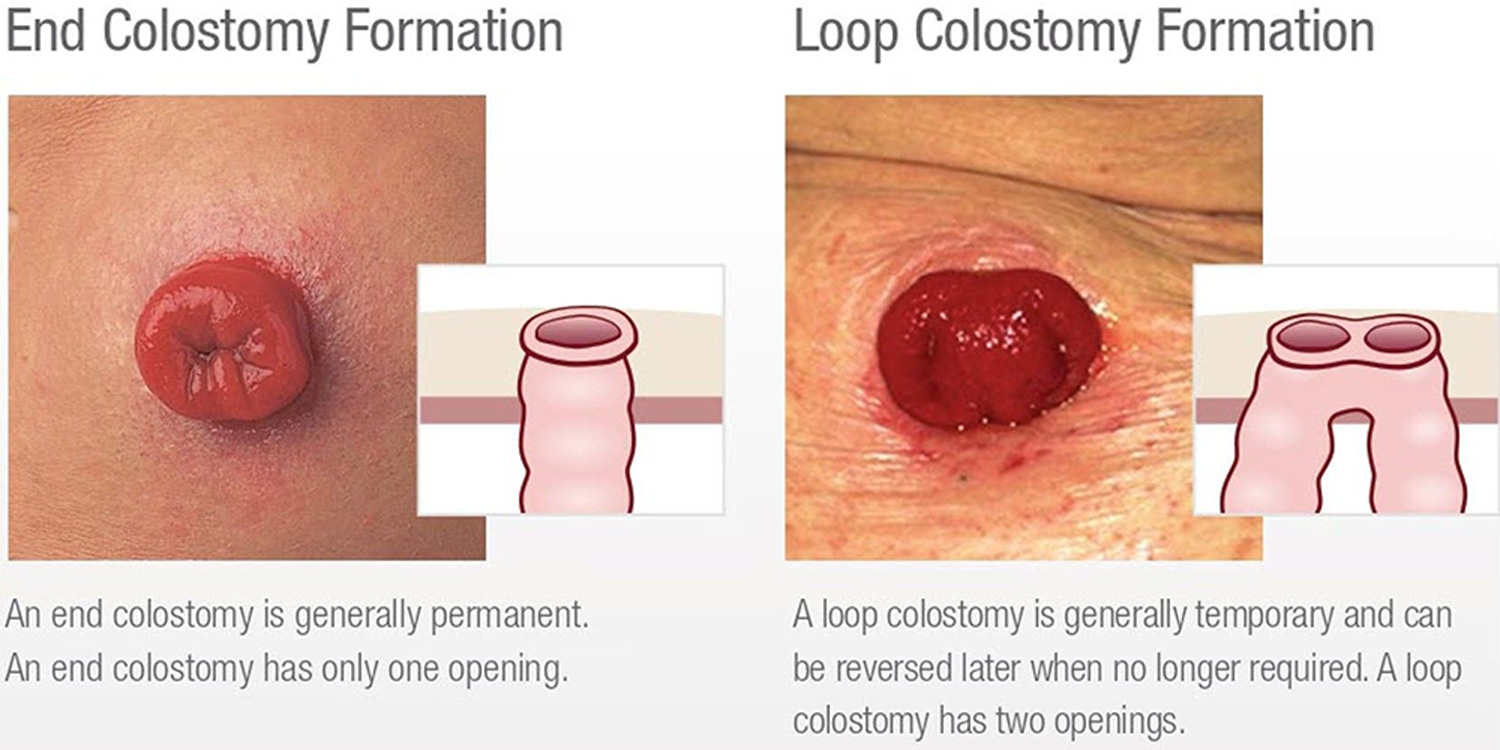
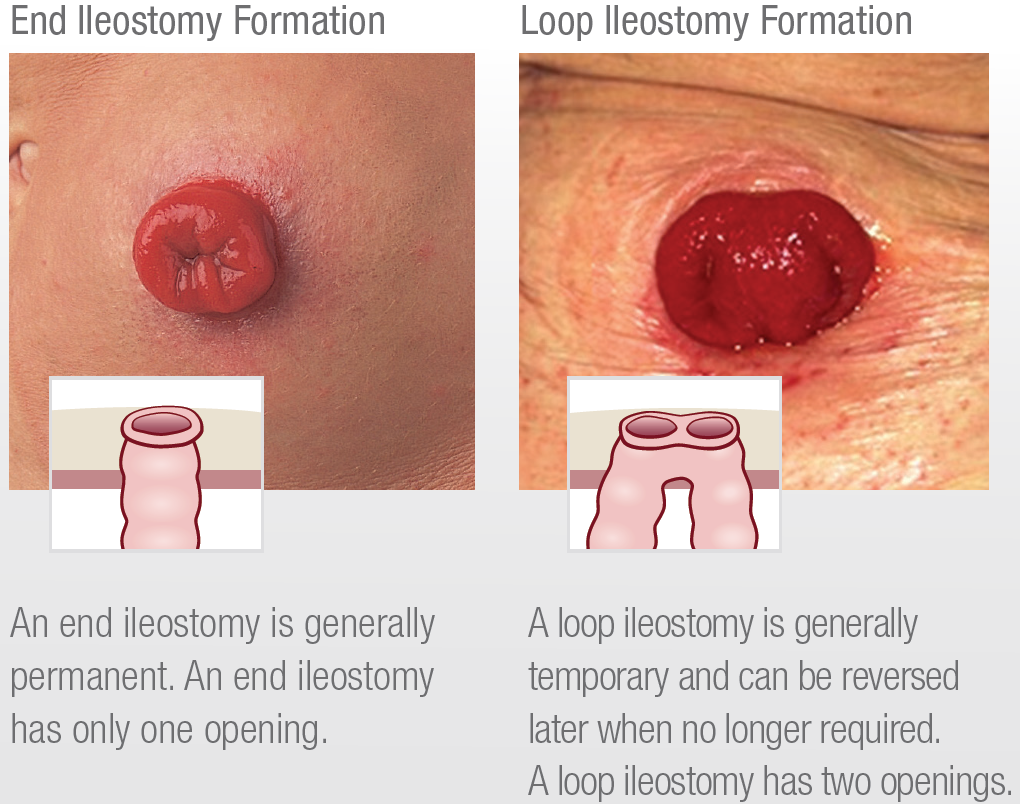
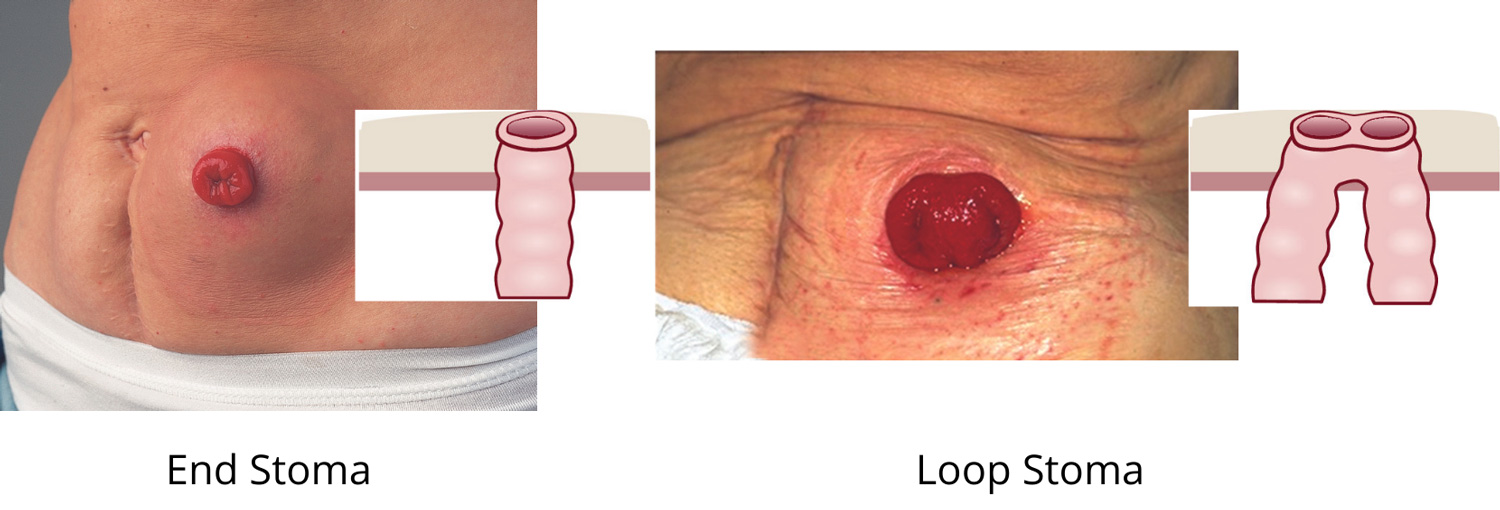
Stoma means “mouth, opening”. Following ostomy surgery, it refers to the small piece of bowel which has been brought to the skin surface of the abdomen. To form a stoma, the surgeon folds back the piece of bowel brought to the abdomen like a cuff on a turtleneck.
Characteristics of a Stoma
Size – varies with each person and type of surgery. Initially after surgery, the stoma is swollen. It will shrink in size as it heals for up to 2 months after surgery. The stoma can get larger with weight gain or if a parastomal hernia develops.
Shape – round, oval, or irregular; raised, flush or retracted stoma on abdomen.
Color – pink to red. The blood supply is very close to the surface of the stoma. It is normal to see traces of blood when the stoma is cleaned or rubbed.
Texture – moist and smooth like the tissue inside your mouth.
Sensation – no feeling in the stoma because there are no nerve endings. If skin around the stoma is irritated, there may be tenderness or pain.
Location – depends where in the bowel the stoma is created and the anatomy of the patient.
Output– depending on the type of ostomy, there will be movement of stool, gas, or urine. It will be involuntary – there is no control.
Stitches – may or may not be seen around the base of the stoma. They usually dissolve in 7 to 10 days.
Peristalsis – slight movement of the stoma may be seen as waste passes through the bowel and stoma.
Rod or bridge – the surgeon may use a plastic rod or tube to support a loop type stoma during the first 1 to 2 weeks, then it is painlessly removed.
May be permanent or temporary
additional guides
Guide to living with a jejunostomy
Credit: Nurses Specialized in Wound, Ostomy and Continence Canada